She Knew It Was Breast Cancer. So Why Didn't Doctors Believe Her?
“Hearst Magazines and Verizon Media may earn commission or revenue on some items through the links below.”
Six years ago, Jessica Florence’s then boyfriend noticed a lump in her breast. “I could see [it] coming out of my shirt,” she says of the moment she knew she needed to seek medical help. “You know your body; you know when something’s not normal.” From 2015 to 2016, Florence, then 21, visited two doctors. Both told her it was just fibroids. She kept getting the same feedback: “You’re too young to have breast cancer.” It wasn’t until Florence, a Black woman and architecture student from Jacksonville, Florida, got new insurance and finally saw another doctor, who ordered a biopsy and ultrasound, that she was diagnosed with breast cancer. It was Stage IIIA, a more advanced form that indicates it has spread to the lymph nodes.
Research from the American Cancer Society shows that while Black and white women are diagnosed with breast cancer at similar rates, Black women are more likely to be diagnosed both at younger ages and at later stages of the disease. They are also 40 percent more likely to die from breast cancer. “Disparities in cancer outcomes and cancer care have historically been attributed to access,” says Dorraya El-Ashry, PhD, the chief scientific officer at the Breast Cancer Research Foundation. “You can’t get to the doctor, you can’t afford the medicine, you’re working four jobs, you don’t have time, and you can’t pick up your medicine for whatever reason. ” Access, she says, is the term broadly used to refer to the seen and unseen barriers Black breast cancer patients come up against. “Access is not just getting to the doctor and the doctor diagnosing breast cancer correctly,” El-Ashry explains. “It encompasses the entire treatment process and the outcome of breast cancer for [Black] women.”
Diving more deeply into this subject is Andrea Silber, MD, an expert in breast cancer among African American women and the assistant clinical director for Health Equity and Diversity at the Yale Cancer Center. “I see [medical] students write things like ‘Well, she didn’t take her meds’ or ‘She no-showed.’ It doesn’t take into account how the patient lives, the struggles she may have,” Silber says. “How can you get to a hospital? Who can afford to drive you? Who can afford to miss work? What happens to your kids? All these things are part of it...but they’re considered irrelevant by most of the medical community.”
Breast cancer is rarely found in someone of Florence’s age, and that likely was a factor in doctors dismissing her symptoms. But systemic medical racism, often manifested in doctors’ unwillingness to hear Black patients’ concerns, is also crushingly pervasive—and can be deadly.
Even when it comes to breast cancer research, Black women are not well represented. Many are reluctant to enroll in clinical trials. Some experts attribute their reticence to fear—a psychological effect of America’s long history of experimenting on and exploiting Black bodies. A 2016 study in Cancer Control posited that low participation in clinical studies could be due to a lack of awareness of current trials, costs to patients, and limited resources at hospitals serving communities of color. Underrepresentation slows down advances in care for Black patients, increasing racial disparities in cancer outcomes and survival. It ultimately means that doctors don’t have a good understanding of how cancer uniquely affects and should be treated in Black patients. The difference is so marked that this year the Basser Center for BRCA at the Abramson Cancer Center of the University of Pennsylvania launched a new initiative to improve awareness and participation of Black patients in breast cancer studies.
Beyond data, conscious and unconscious bias across the medical community is life-threatening to patients, regardless of their socioeconomic status. Florence had the advantages of access to health care and wonderful family support, and the system still failed her. After Serena Williams gave birth to her daughter in 2017, medical staff ignored her concerns about blood clots—and nearly missed the pulmonary embolism she was experiencing.
Bias in care can be seen on a small scale, right in the waiting room. “I look at brochures,” Silber says. “All the women in the pictures are skinny and blonde. What does that say?”
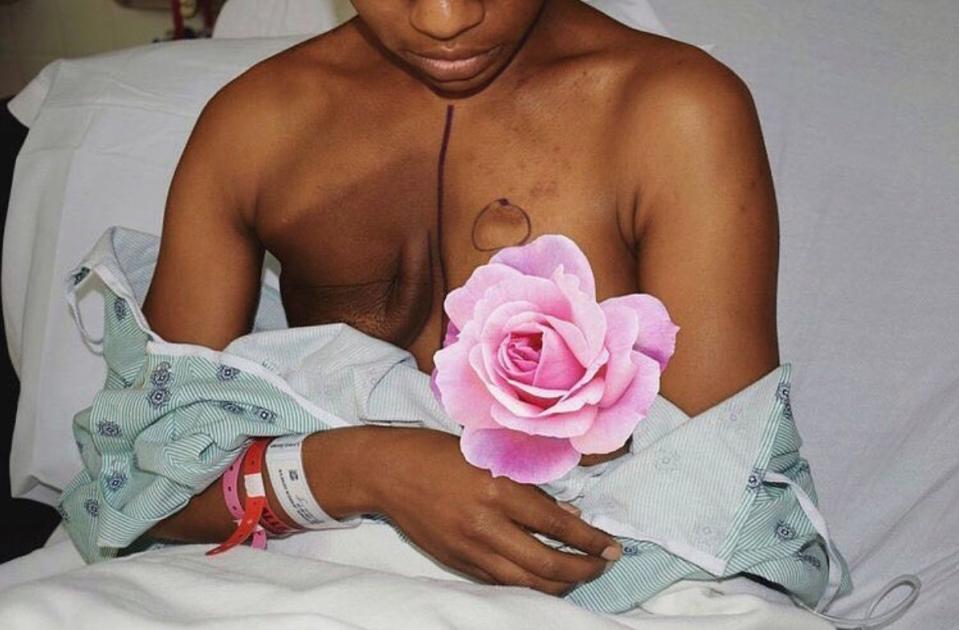
Florence felt this lack of representation firsthand. When she was first diagnosed, she went online to see what a double mastectomy would look like on her dark skin. Her search turned up only minimal results. After surgery, she posted her images so that other women of color could see themselves. “I couldn’t go on Google and see what my skin was going to look like after a Herceptin treatment, so that’s why I posted my pictures,” Florence says. “I hope it helps people get through it a little faster and feel more prepared.” Silber echoes this sentiment, pointing out that while we know chemotherapy causes hair to fall out (because the drugs attack fast-dividing cells), far fewer people are aware that it affects Black women’s nails, often turning them dark, an effect known as melanonychia.

On a larger scale, the consequences of bias become even more sobering. A 2016 study on racial bias in pain assessment found that the old falsehood that Black patients feel less pain than their white counterparts still exists. In the August issue of the New England Journal of Medicine, Oluwafunmilayo Akinlade, MD, addressed the persistent problem in an article titled “Taking Black Pain Seriously”: “Remember that you can harbor these biases even if you believe that all races are equal,” she warned her fellow caregivers.
Critical to breaking these patterns is speaking directly to Black women and, more importantly, listening, says Silber, who launched an initiative at Yale to provide outreach to the Black community in New Haven, Connecticut. “If you’re doing things that don’t seem like they are being thought about from other people’s perspective, it’s not going to go over well,” she says. “They need to be equal stakeholders.” The four-year-old initiative, called Oncologists Welcome New Haven Into Trial (OWNIT), aims to meet institutional needs for research while prioritizing community needs, such as funding hospitals and programs.
After over a year of misdiagnoses and then ultimately fighting the disease (six rounds of chemotherapy, radiation, and a unilateral mastectomy), Florence finished her treatments in 2017 with an “All clear.” That should have been it: Wrap it up and make way for the queen. But two years later, she suddenly became plagued by headaches, sending her cancer intuition into overdrive. Visits to multiple doctors left her with a sense that no one was taking her seriously. Again. “I’m telling these people I have a headache, I’m vomiting, I’m having a lot of nausea and I have a history of breast cancer,” she says. “Once you hear those symptoms, somebody should automatically put you on an MRI table or get you a CT, a PET scan.” Instead, she heard a wretchedly familiar refrain: “Headaches are normal.” “What’s your diet?” “I don’t think it’s a brain tumor; it’s just stress or lack of sleep.”

Still, she knew her own body. In April, Florence learned that the cancer originally in her breasts had metastasized. After two fruitless visits to the ER, she had gone in again and told the attending physician her symptoms. “He was like, ‘Okay, Miss Florence, I’m going to have to put you on the MRI table, because something’s not right,’ ” she recalls. “Ten minutes later, he was like, ‘We’ve got to do emergency surgery. You have two tumors in your head. Your breast cancer has metastasized.’ ” She now had Stage IV breast cancer that had spread to her brain. At 26, she is facing a second—and more serious—battle with cancer and wondering if she will have to second-guess every minute of care she gets along the way.
In 2020, almost every system and institution is looking at internal racism, but few more urgently require that reflection than the medical community. “It’s not something in the DNA that has caused Black women to do worse with breast cancer,” Silber says. “So much of what has been funded and what people have looked for is very microscopic, very cutting-edge scientific reasons [for the discrepancies in cancer outcomes] that definitely have to do with social determinants of health.” But what it’s not addressing are years of systemic discrimination playing itself out on Black bodies. It’s not, she says, “looking at what’s right in front of our eyes. It’s racism. It’s been that way forever.”
This article appears in the October 2020 issue of ELLE.
You Might Also Like
